Surgery for shoulder calcific tendinitis may be considered when the calcium deposit is larger than 10mm or pain persists for over 8 months. However, a cautious approach is necessary as pain can continue post-surgery for months, and there's a risk of developing frozen shoulder.
When to Consider Surgery for Shoulder Calcific Tendinitis?
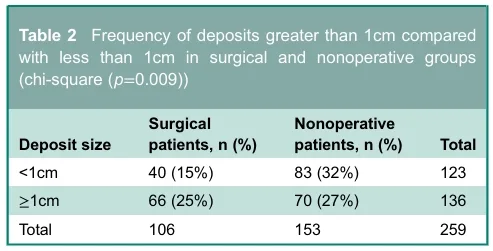
Shoulder calcific tendinitis, which causes sharp, stabbing pain, is a common condition, but not all patients require surgery. Clinical studies indicate that while larger calcium deposits, exceeding 10mm, are more likely to necessitate surgery, many cases larger than 10mm can still be managed with conservative treatments. Therefore, the size of the calcium deposit is a significant factor but not an absolute determinant for surgery. Surgery might also be considered if pain persists for over 8 months or if non-surgical treatments like injections and physical therapy provide only temporary relief before symptoms return. A trend shows a higher rate of surgery among female patients. The crucial factor is not just the intensity of pain but a comprehensive assessment of its duration and pattern.
What to Expect Post-Surgery: Reality vs. Expectations
Surgery for calcific tendinitis often involves more than just removing the calcium deposit. Procedures like arthroscopic debridement, rotator cuff repair, subacromial decompression, and capsular release may be performed concurrently. Post-surgery, steroid injections might be used adjunctively for pain management. Approximately 11.3% of patients may develop frozen shoulder (adhesive capsulitis) after surgery, and pain can persist for an average of 5 to 6 months. Patients might experience temporary limitations in shoulder movement, particularly with external rotation. It's essential to have realistic expectations about the recovery process, understanding that surgery isn't always a simple 'fix' but the beginning of a recovery journey.
Who is More Likely to Fail Non-Surgical Treatments?
Identifying patients who are more likely to experience failure with non-surgical treatments is key. Research suggests that individuals with calcium deposits larger than 10mm, pain lasting over 8 months, or those who show only transient improvement with injections or physical therapy are more likely candidates for surgery. Female patients also tend to have a higher rate of progressing to surgery. A comprehensive evaluation of these predictive factors is necessary to tailor the optimal treatment plan for each individual. Consulting with a specialist is highly recommended for an accurate diagnosis and personalized treatment strategy.
Are There Non-Surgical Management Options for Calcific Tendinitis?
Non-surgical management for calcific tendinitis includes various approaches. Initially, over-the-counter pain relievers, physical therapy, and extracorporeal shockwave therapy (ESWT) may be attempted. For acute, severe pain, corticosteroid injections can be effective in reducing inflammation. Consistent stretching and exercises to strengthen and maintain the flexibility of the shoulder muscles are also crucial. However, if these non-surgical treatments do not provide relief or significantly impact daily life, surgical intervention may be considered.
For more details, check the original source below.